

Pimples vs. Boils vs. Cysts: How to Tell What’s on Your Skin
Discovering an unexpected bump on your skin can trigger immediate concern. Is it a harmless pimple, a serious boil requiring medical attention, or a persistent cyst needing professional evaluation? Understanding these distinctions is essential for proper treatment and preventing complications.
In Pakistan’s challenging climate, where temperatures exceed 40°C and humidity reaches 80%, skin conditions occur with increased frequency. The combination of heat, moisture, and bacterial proliferation creates ideal conditions for various skin bumps. This guide will help you accurately identify these conditions and make informed treatment decisions.
Understanding the Conditions: Medical Definitions
Pimples (Acne Lesions):
Pimples are inflammatory lesions affecting the pilosebaceous unit. Research shows that acne affects 85% of individuals aged 12-24, with prevalence remaining significant in adulthood. The pathogenesis involves four mechanisms: sebaceous gland hyperactivity, follicular hyperkeratinization, bacterial colonization by Cutibacterium acnes, and inflammatory cascade activation.
Studies indicate that genetic factors account for 80% of acne susceptibility, while hormonal fluctuations can increase sebum production by 500% during puberty.
Boils (Furuncles):
Boils are deep bacterial infections of hair follicles and surrounding tissue. Unlike superficial pimples, boils extend through multiple tissue layers, creating significant inflammation. Staphylococcus aureus accounts for 80-90% of cases, with methicillin-resistant strains (MRSA) comprising 15-20% of community-acquired infections in urban Pakistan.
Clinical studies show that early antibiotic intervention reduces progression to abscess formation by 60-70%.
Cysts (Sebaceous Cysts):
Sebaceous cysts are benign, encapsulated lesions containing keratinaceous material. Research indicates that complete surgical excision prevents recurrence in 95% of cases, while simple drainage results in 50-70% recurrence rates. These developmental anomalies can occur anywhere but commonly affect the face, neck, and trunk.
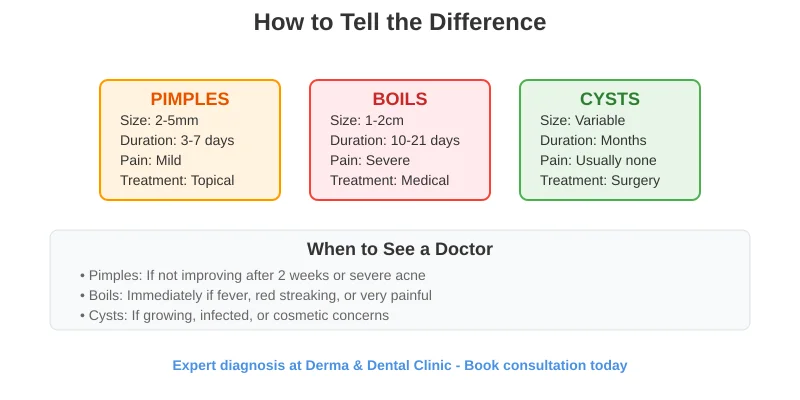
Visual Identification Guide
Identifying Pimples:
- Size: 2-5mm diameter, occasionally reaching 8-10mm
- Color: Red base with possible white, yellow, or black centers
- Location: Face, chest, back, shoulders (sebaceous-rich areas)
- Texture: Soft to moderately firm, often fluctuant when containing pus
Types:
- Comedones: Blackheads and whiteheads (non-inflammatory)
- Papules: Small, red, solid bumps
- Pustules: Inflamed lesions with visible pus
- Nodules: Large, deep, painful lesions
Timeline:
- Development: 2-3 days from onset to visible lesion
- Peak inflammation: 3-5 days
- Resolution: 7-14 days with proper care
- Post-inflammatory changes: Erythema may persist 2-8 weeks
Identifying Boils:
Primary Features:
- Size: Initially 1-2cm, expanding to 5cm if untreated
- Color: Deep red to purple with central yellow/white pointing
- Location: Friction-prone areas (buttocks, thighs, axilla, neck)
- Texture: Extremely firm with significant surrounding swelling
Clinical Stages:
- Initial phase (Days 1-3): Small, painful red nodule
- Development (Days 4-7): Rapid enlargement with central softening
- Pointing (Days 7-10): Central fluctuance with visible pus
- Resolution (Days 10-21): Drainage or surgical intervention
Associated Symptoms:
- Severe pain and throbbing sensation
- Warmth and tenderness
- Possible fever and malaise in severe cases
- Regional lymph node enlargement
Identifying Cysts:
Primary Features:
- Size: Variable, from 3mm to 10cm diameter
- Color: Skin-colored to slightly yellow/white
- Location: Face, neck, trunk (can occur anywhere)
- Texture: Soft to firm, well-circumscribed, mobile under skin
Characteristic Features:
- Central punctum: Small dark opening occasionally visible
- Mobility: Moves freely with gentle pressure
- Consistency: Firm but compressible, “rubbery” texture
- Pain: Usually painless unless infected
Complication Signs:
- Sudden pain, redness, warmth (infection)
- Discharge of foul-smelling material (rupture)
- Rapid enlargement or change in consistency
Causes and Risk Factors
Pimple Development:
Hormonal Factors: Research demonstrates that androgens increase sebaceous gland size 4-5 fold during puberty. Hormonal fluctuations cause flares in 65% of women, typically 7-10 days before menstruation.
Environmental Factors:
- High humidity increases bacterial proliferation by 300%
- High-glycemic foods increase IGF-1 levels by 15-20%
- Comedogenic cosmetics contribute to adult female acne
- Mechanical friction causes acne mechanica
Boil Development:
Bacterial Factors: Staphylococcus aureus causes 85-90% of uncomplicated boils. MRSA prevalence is increasing in community settings, particularly in urban Pakistan.
Risk Factors:
- Diabetes mellitus: 3-fold increased risk
- Immunosuppression from medications or conditions
- Poor hygiene and compromised skin barrier
- Crowded living conditions increasing transmission
Climate Factors:
- Temperature extremes impair immune function
- 70-80% humidity promotes bacterial growth
- Air pollution disrupts skin barrier function
Cyst Development:
Developmental Factors:
- Follicular occlusion preventing normal desquamation
- Genetic predisposition (affects 15-20% of population)
- Hormonal influences stimulating sebaceous activity
Acquired Factors:
- Physical trauma implanting epithelial cells
- Previous surgical procedures with inadequate wound care
- Chronic inflammatory conditions
Treatment Approaches
Pimple Treatment:
- Benzoyl peroxide 2.5-5%: Reduces bacteria by 99% within 2 weeks
- Salicylic acid 0.5-2%: Beta-hydroxy acid with comedolytic properties
- Retinoids: Adapalene 0.1% or tretinoin 0.025-0.1%
- Combination therapy: Morning benzoyl peroxide, evening retinoid
Systemic Options:
- Antibiotics: Your dermatologist may prescribe daily or at alternative days for anti-inflammatory effects
- Hormonal therapy: Oral contraceptives or spironolactone for women
- Isotretinoin: 0.5-1.0 mg/kg/day for severe cases
Professional Procedures at Derma & Dental Clinic:
- Comedone extraction with sterile technique
- Chemical peels for active acne and scarring
- Light therapy targeting bacterial colonization
Boil Treatment:
Conservative Management:
- Warm compresses 15-20 minutes, 4-6 times daily
- Pain management with NSAIDs
- Antibacterial soap and separate personal items
- Avoid squeezing or attempting drainage
Antibiotic Therapy:
- First-line: Cloxacillin 500mg four times daily
- MRSA coverage: Doxycycline 100mg twice daily
- Severe cases: Linezolid 600mg twice daily
Surgical Intervention at Derma & Dental Clinic:
- Incision and drainage: For fluctuant boils >5cm
- Technique: Cruciate incision with complete drainage
- Success rate: 95% resolution with single procedure
- Follow-up: Wound checks at 48 hours, 1 week, 2 weeks
Cyst Treatment:
Observation vs. Treatment: Small, asymptomatic cysts may be monitored. Treatment indicated for cosmetic concerns, functional impairment, or recurrent infection.
Surgical Options at Derma & Dental Clinic:
- Complete excision: Gold standard with <5% recurrence rate
- Minimal excision technique: Smaller scar, 10-15% recurrence
- Infected cyst management: Initial drainage, delayed excision after inflammation resolves
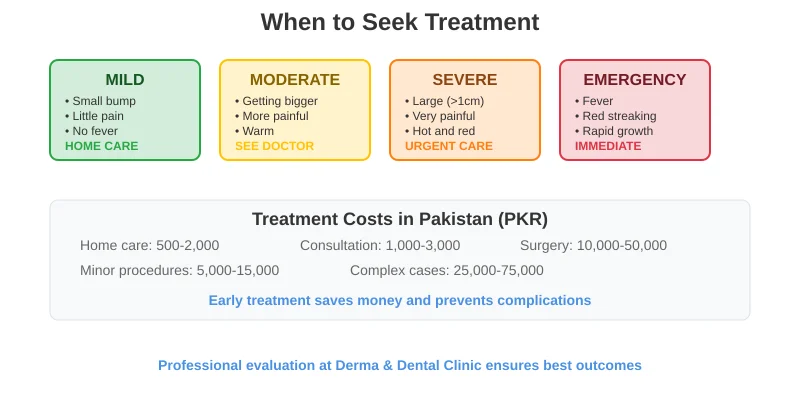
Always Seek Professional Help:
- Fever or chills with skin lesion
- Red streaking from the bump
- Rapid enlargement over 24-48 hours
- Severe pain interfering with daily activities
- Facial boils (risk of complications)
Routine Evaluation:
Schedule Consultation When:
- Uncertain about lesion identity
- No improvement after appropriate treatment
- Recurrent episodes
- Cosmetic concerns or scarring risk
- Multiple lesions appearing simultaneously
Visit Derma & Dental Clinic for comprehensive evaluation, accurate diagnosis, and personalized treatment plans using advanced techniques and proven protocols.
Prevention Strategies:
Skincare Fundamentals:
- Gentle cleansing twice daily with non-comedogenic products
- Moisturize with hyaluronic acid-based formulations
- Use broad-spectrum SPF 30+ daily
- Avoid touching face and pick lesions
Hygiene Protocols:
- Individual towels and pillowcases changed twice weekly
- Clean phones, makeup brushes, and eyeglasses regularly
- Wear breathable fabrics and wash promptly after sweating
Climate-Specific Care:
- Use air conditioning to reduce humidity and bacterial growth
- Shower immediately after sweating
- Apply lighter moisturizers in humid weather
- Protect from air pollution with barrier products
Conclusion:
Distinguishing between pimples, boils, and cysts is crucial for appropriate treatment and optimal outcomes. While pimples often respond to proper skincare, boils require prompt medical attention to prevent complications, and cysts may need professional evaluation for best results.
Pakistan’s challenging climate creates unique considerations for skin health, making professional guidance particularly valuable. Early intervention improves treatment success rates while preventing complications, scarring, and psychological distress.
If you’re uncertain about any skin bump or experiencing persistent problems, consult our experienced dermatologists at Derma & Dental Clinic. We provide comprehensive evaluations, advanced treatment options, and personalized care plans designed for optimal results in Pakistan’s unique environment.
Book your consultation today to receive expert diagnosis and evidence-based treatment from Pakistan’s leading dermatological specialists.